A 40 yr M with pain in right hypochondrium since 2 days associated with fever
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Here is a case i have seen:
Case history:
40 year old man - carpenter by occupation
Presented to our hospital with complaints of --------Fever high grade since 3-4 days , continuous, associated with chills and rigors
-- pain abdomen - @ Right upper quadrant since 2 days ,radiating to back , gradually progressive
Severe in intensity
Assosciated with 2 episodes of vomitings- non bilious,non projectile , containing food particles and water
He also complaints of burning micturition since 2 to 3 days
No h/o loose stools ,hematemesis ,no obstipation ,no constipation ,no pedal edema ,no abdominal distension .
Not a k/c/o DM,HTN,Asthma, Lymphadenopathy,CAD.
He is a chronic alcoholic since 18-20years - drinks daily 180 ml-500 ml of whiskey daily.
Last alcohol binge was 5 days back .
Chronic smoker since -15 -20 years - smokes 1 beedi pack /day .
Past history:
History of hospitalisation 4 years back with similar complaints - and dark colored stools.He was said to have liver infection back then.
On examination -
Pt is conscious,coherent,cooperative
Oriented to time,place and person.
He is thin built .
Icterus +
Clubbing +
Tremors +


No signs of Pallor,cyanosis, lymphadenopathy,koilonychia,edema.
Febrile - continuous fever spikes since yesterday.


Vitals
Bp- supine - 130/100 mmHg
Standing -100/80 mmHg
PR- 112/min
Spo2-99%
Temp-102 F
Grbs-108mg/dl

Systemic examination:
CNS-Normal.
CVS-s1s2 heard, no murmurs.
RESP SYSTEM- BAE +
Per abdomen -
Umbilicus -normal central in position.
Tenderness at the right hypochondriac region .
Liver span - 17 cms.
No splenomagaly
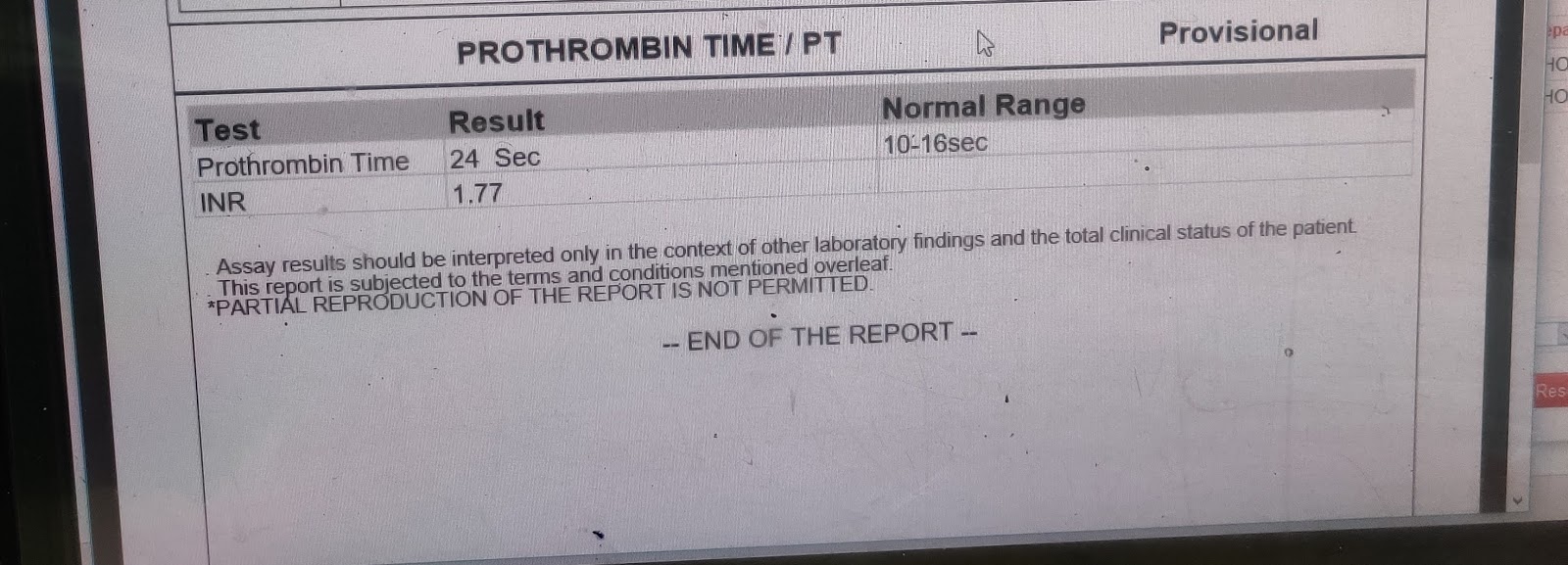
INVESTIGATIONS











Day 2







Usg abdomen-



Provisional diagnosis :
Viral PYREXIA with thrombocytopenia- resolving
Hepatocellular jaundice.
? Acute Hepatitis
Thrombophlebitis +
Treatment:
Day 1
Inj.Monocef 1gm/IV/bd
Inj. Metrogyl 500mg /IV /TID
Inj. Pan 40mg/ IV /od
Inj. Zofer 4mg /IV /tid
Sup.Hepamerz 15ml/po/od
IV fluids- NS and RL
Tab MVT /po /od
Inj. Tramadol 1 amp in 100 ml NS IV
Syp.Lactulose 15 ml BD- to pass 3 to 4 stools/day
Tab. Udiliv 300mg /PO /BD
Sup. Hepamerz 15ml / PO H/S.
Tab.Ultracet /po/qid
Tepid sponging- for fever
Day 2
Inj.Monocef 1gm/IV/bd
Inj. Metrogyl 500mg /IV /TID
Inj. Pan 40mg/ IV /od
Inj. Zofer 4mg /IV /tid
Sup.Hepamerz 15ml/po/od
IV fluids- NS and RL
Tab MVT /po /od
Inj. Tramadol 1 amp in 100 ml NS IV
Syp.Lactulose 15 ml BD- to pass 3 to 4 stools/day
Tab. Udiliv 300mg /PO /BD
Sup. Hepamerz 15ml / PO /od
Tab.Ultracet/po/qid
Day 3
Inj.Monocef 1gm/IV/bd
Inj. Metrogyl 500mg /IV /TID
Inj. Pan 40mg/ IV /od
Inj. Zofer 4mg /IV /tid
Sup.Hepamerz 15ml/po/od
IV fluids- NS and RL
Tab MVT /po /od
Inj. Tramadol 1 amp in 100 ml NS IV
Syp.Lactulose 15 ml BD- to pass 3 to 4 stools/day
Tab. Udiliv 300mg /PO /BD
Sup. Hepamerz 15ml / PO H/S
Tab.Lasix 40 mg /po/bd
Tab.Ultracet/po/qid
Tab.Ondansetron 4mg/po/sos
Day 4
Inj.Monocef 1gm/IV/bd
Inj. Metrogyl 500mg /IV /TID
Inj. Pan 40mg/ IV /od
Inj. Zofer 4mg /IV /tid
Sup.Hepamerz 15ml/po/od
IV fluids- NS and RL
Tab MVT /po /od
Inj. Tramadol 1 amp in 100 ml NS IV
Syp.Lactulose 15 ml BD- to pass 3 to 4 stools/day
Tab. Udiliv 300mg /PO /BD
Sup. Hepamerz 15ml / PO H/S.
Tab.Thiamine 100mg/po/od
Tab.Lasix 40 mg /po/bd
Tab.Ultracet/po/qid
Tab.Ondansetron 4mg/po/sos


Comments
Post a Comment